{kind=link}
Ruth Nekesa (Not her real name) wakes before dawn in her two room house in Mjini, a slum estate in Bungoma town.
The first thing she does, even before lighting her charcoal jiko, is reach for the small plastic bottle on a wooden stool across her bed.
She takes out antiretroviral pills and swallows them with water from a plastic bottle by her bedside. No food yet. That will come later, if there’s enough.
By 7:00m AM on a Monday, she needs to be going to the hospital.
On a normal day, she could walk to the hospital, but today, a 10 minute motorbike led her to arrive earlier.
At 8:15 AM, she is at the Comprehensive Care Centre at the Bungoma County Referral Hospital.
The waiting bay is already crowded. Patients sit shoulder-to-shoulder on wooden benches, some stare at their phones others close their eyes, resting.
Ruth finds a spot near the door and settles in, pulls her cardigan tighter and waits.
She has been coming here for two decades, if all goes well, she’ll leave with a three-month supply of antiretrovirals.
If not, she doesn’t let herself think about “if not.”
But today, for the first time in a long time, she is afraid. Not of the virus. But what happens when the system that keeps her alive stops working.
Her story is a testament to the the ripple effects quietly unfolding across Kenya’s public health system after the United States announced the withdrawal of its health support in January 2025.
Funding freeze
When news broke that USAID, the American agency that had funded her treatment for years, was pulling out, she shuddered with fear: “The first thing I thought about was death,” she says, with her calming voice. “I knew I could no longer access the drugs.”
Ruth knows exactly what happens when the medicine stops.
Years ago, she walked away from her treatment for two years.
She says; “I watched my health deteriorate, but since resuming taking the drugs, I have found stability and life again.”
Duncan Wanyonyi (not his real name), is haunted by a different kind of memory.
He is living with HIV, while navigating life with his HIV-negative wife.
For him, the announcement of the funding cuts felt like a rewind to a time he thought Kenya had left him behind.
He remembers the years between 2003 and 2005, the era before massive donor support made ARV’s free at the point of care. He says, during that time,
“The first question was, how much I was going to pay.” he says “I am still not confident on what will happen in the future”, he adds.
The withdrawal had a serious impact on many patients in Bungoma.
As the HIV coordinator Bungoma County, Joy Nyarotso says, for weeks, they had to follow up with other patients to come for the drugs because the majority had given up accessing the drugs.
“We had to follow up most patients to come for their checkups and drugs because of the information that drugs were no longer available, and there was no communication on way forward” she says
She says that USAID did not just support giving drugs, it also supported counseling and follow ups assistance and structure.
However, even before the US withdrawal, Kenya’s HIV response was experiencing gaps.
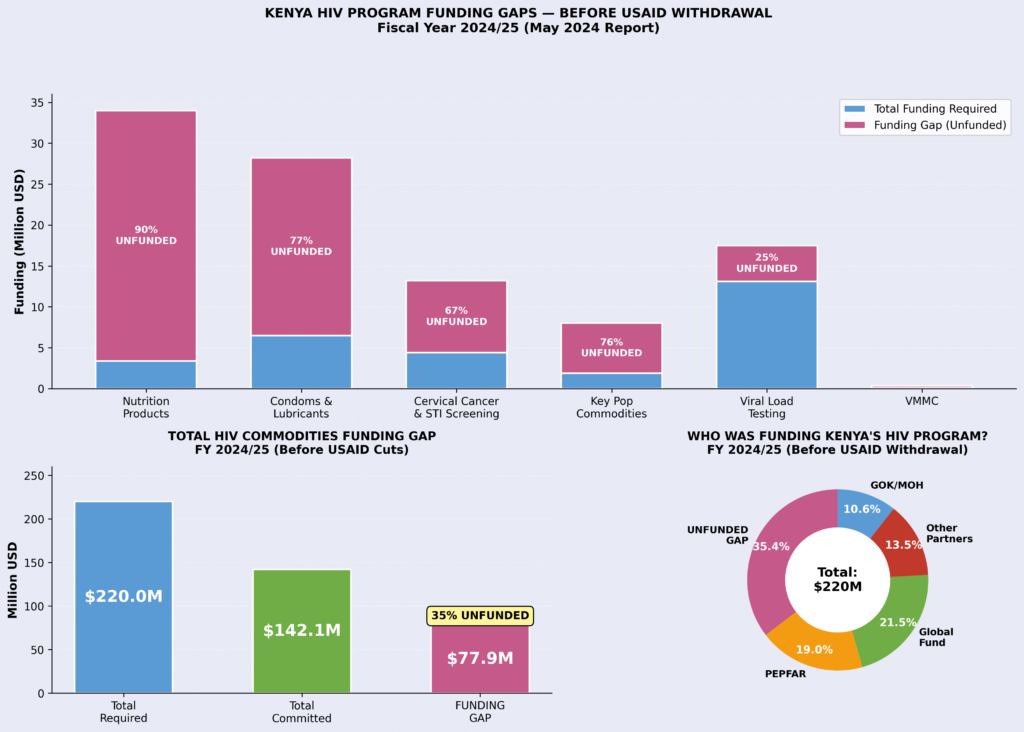
A National Quantification Report for HIV Commodities for FY 2024/25 to 2026/27 by National AIDS and STI Control Program (NASCOP) in March 2024 revealed a funding gap of USD77.9 million for HIV commodities, which represent 35 per cent of the total need unfunded.
According to the report, nutrition products for malnourished HIV patients were 90 per cent unfunded, Condoms were 77 per cent unfunded with services for key populations including sex workers, were 76 per cent unfunded.
Under Kenya’s devolved health system, counties are responsible for the Human Resources for Health (HRH), and the operational costs of health facilities.
However, the transition from donor to County responsibility has been a story of fiscal avoidance: “The reluctance of County governments to absorb donor-funded staff has created a lethal gap in human resources,” notes Ignatius Nyukuri, a health budget advocate.
He adds that: “The biggest challenge is with the budget process, with most cases County governments failing to allocate relevant funds to important departments, and only focusing on recurrent budgets instead.”
Despite years of warnings that donor support was not reliable, counties budget allocations have largely failed to secure funds for HIV continuity.
Bungoma County HIV funding
While Bungoma County’s Programme Based Budget (PBB) for FY 2024/25 lists millions for medical supplies and infrastructure, the specific technical costs of maintaining a HIV programme, such as reagents for viral load tests and transport for sample monitoring, often remain invisible or underfunded.
Benjamin Otsiula, the County Assembly chair of the Budget Committee agrees that there is a lack of strategy for donor exit, both in the local and national government.
“You cannot set a ceiling and you want to factor in funds that you don’t have. You set ceilings according to, first of all, your own source revenue,” he says
Relating to the County Governments 2024/2025 and 2025/2026 budgets, Otsiula attests that without donor funding in the health sector, it is not possible for the local governments to sustain themselves.
“The easiest thing, at least when the budget is being submitted, HIV related programmes are supposed to be captured. It’s not difficult.” he adds
A report from Bajeti Hub’s County Budget Transparency Survey 2024 opines that while county transparency is improving, meaningful accountability is still blocked by gaps in detail and public participation reporting.
The survey reports an overall score of 64/100, with counties publishing 84 per cent of the key budget documents assessed, yet still failing to provide 39 per cent of the information required by law.
Nyukuri says it is a violation of the spirit of the Public Finance Management (PFM)Act, which requires budgets to be credible and based on actual service needs.
According to the National and County Health Budget Analysis for the 2023-2024 financial year, Kenya’s health system depends heavily on foreign aid, which provides nearly a third of the national budget, amounting to about Sh21.5 billion.
The 2025/2026 budget of Sh4.29 trillion is below the Ksh643.5 billion recommended by the Abuja Declaration of 2001, in which governments were to scale health budgets to 15 per cent of total budgetary allocation.
The government allocates far less than needed for healthcare, with health economists and public health experts stating that the country has poorly funded public healthcare system spending only USD38 (Ksh4,800), annually for each of its people a far cry from the recommended USD86 (Ksh10,900), resulting in persistent poor healthcare and unhealthy donor dependence.
Analysis based on U.S foreign assistance to Kenya states HIV/AIDS programmes received the lion’s share of USAID health funding in Kenya, accounting for nearly 60 per cent of the USD278.5 million allocated in 2024
Timothy Kiprono, a public finance and governance expert at the Institute of Public Finance argues that the withdrawal of USAID funding did not create the crisis, but exposed it.
“This is a case of healthcare not being just like any other sector,” he explains. “If you anchor a statutory obligation like healthcare on an unsustainable funding source, then you’re risking the lives of Kenyans.”
For years, donor funding, particularly through USAID, quietly carried critical parts of Kenya’s HIV response leading to strengthening existing government systems,
“USAID showed clearly that we are delegating our responsibility as a country to well-wishers,” he adds, “The impact was both financial but also capacity. It is not just that we don’t have money, we also lost the system to deliver services.”
In December 2025, Kenya and the US signed a major health partnership agreement investing USD1.6 billion (Sh208 billion) over five years to make Kenya‘s health system sufficient by 2031.
Kenya will contribute about Sh850 million over the five years, with the U.S. providing USD1.6 billion, with money going directly to the government, bypassing non-governmental organizations that were previously handling programmes like HIV in Kenya.
Even after USAID’s withdrawal, Kenya continued to rely heavily on foreign aid.
In the 2025/2026 financial year, the largest commitments for healthcare development came from donors including the Susan Thompson Buffett Foundation, the Global Fund, and the Global Alliance for Vaccines and Immunization (GAVI).
With these donors showing inconsistent support in previous years, there are still concerns about sustainability of the programmes.
For Bungoma, and other Counties, the lessons require urgent addressing.
Healthcare cannot be sustained on temporary goodwill. Without deliberate planning, budgeting, and integration of donor support into national and county systems, each withdrawal risks becoming not just a funding gap but a public health crisis.
As Timothy puts it, the solution is not simply more money, but better systems.
He says: “Donor support should build systems and transfer capacity so that when they leave, the government continues without disruption.”
Until then, the waiting bay at the Comprehensive Care Centre will continue to tell a story not just of illness but of a system struggling to stand on its own.